
Microdosing Semaglutide Chart: A Monthly Dose Guide For Josie Patients
A semaglutide microdosing chart that supports comfort, longevity, and gentle month-to-month increases.
This is some text inside of a div block.
July 23, 2025
Tirzepatide vs. semaglutide for GLP-1 microdosing, midlife maintenance, and healthy habits.

The Josie Team
Medically Reviewed by

This content is for educational purposes only and is not medical advice. GLP-1 microdosing is not an FDA-approved dosing category and has not been evaluated in large randomized clinical trials. Compounded GLP-1 medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality. A licensed provider must review your health history before any prescription is written. Individual results vary.
Tirzepatide and semaglutide may feel different at lower doses because they work through different pathways, but there’s no large clinical trial evidence proving that one is better than the other for microdosing.
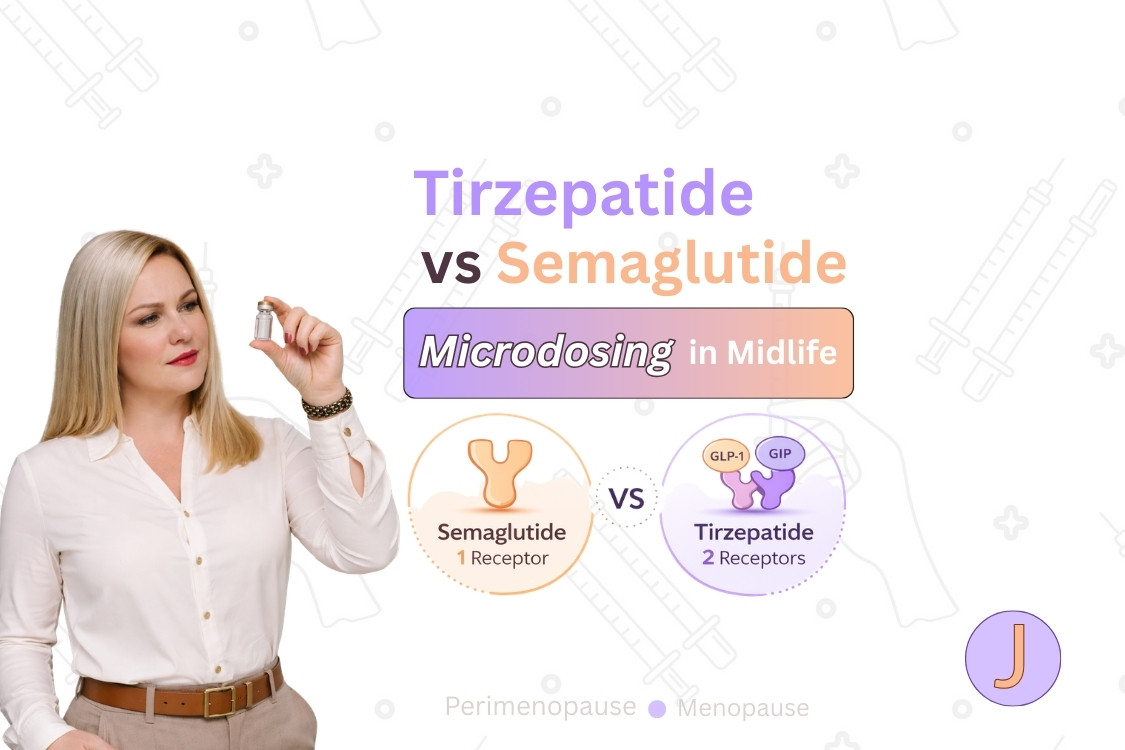
Semaglutide works through the GLP-1 pathway. Tirzepatide works through both the GLP-1 and GIP pathways. That pathway difference may affect appetite, fullness, digestive comfort, or tolerability for some women, but individual response is hard to predict.
At Josie, GLP-1 microdosing is used for weight maintenance and longevity support, not active weight loss. It may be considered for women who’ve reached a stable weight or who are already at a comfortable weight and want provider-guided support during midlife changes.
Microdosing isn’t an FDA-approved dosing category. Compounded GLP-1 medications aren’t FDA-approved and haven’t been evaluated by the FDA for safety, effectiveness, or quality.
A licensed provider should review whether microdosing fits your health history, current weight status, medications, side-effect history, risk factors, and maintenance goals.
Tirzepatide and semaglutide are related medications, but they aren’t interchangeable.
Semaglutide is a GLP-1 receptor agonist. Tirzepatide is a dual GIP and GLP-1 receptor agonist. Both medications have been studied at standard treatment doses, but microdosing hasn’t been studied the same way.
The practical takeaway is simple: tirzepatide and semaglutide may feel different, but the evidence doesn’t support ranking one as the better microdosing option.
Dosing charts:
No large clinical trial evidence proves that tirzepatide is better than semaglutide for microdosing.
Tirzepatide works through both GIP and GLP-1 pathways. Semaglutide works through the GLP-1 pathway. That difference may affect how each medication feels, but microdose-level outcomes aren’t well established.
At lower doses, one woman may notice steadier appetite. Another may notice digestive sensitivity. Another may notice little change. A licensed provider should review the full health picture instead of choosing based on pathway alone.
Semaglutide and tirzepatide may feel different at lower doses because they activate different incretin pathways.
Semaglutide acts on the GLP-1 pathway. Tirzepatide acts on both the GLP-1 and GIP pathways. That pathway difference may affect appetite, fullness, digestion, nausea, constipation, or overall tolerability.
Response can vary based on health history, current weight, appetite patterns, digestive sensitivity, sleep quality, stress, muscle mass, protein intake, strength training habits, other medications, and hormone changes during midlife.
Josie doesn’t frame the choice as “which one is better?” The better question is whether either medication fits the patient’s health history, current weight status, risk factors, and maintenance goals.
Semaglutide and tirzepatide have been studied at standard treatment doses in large clinical trials.
That research helps explain why GLP-1 medications are used in standard care for weight management when clinically appropriate. Standard-dose trial data shouldn’t be treated as proof that microdosing produces the same outcomes.
There isn’t the same level of research on GLP-1 microdosing. Microdosing hasn’t been evaluated in large randomized clinical trials for weight maintenance, longevity support, side-effect thresholds, lean-mass outcomes, or head-to-head comparisons between semaglutide and tirzepatide.
That evidence gap matters. Microdosing should be discussed carefully with a licensed provider, especially when the goal is maintenance rather than active weight loss.
GLP-1 microdosing at Josie is a lower-dose, provider-guided option for women focused on maintaining their weight and supporting healthy habits.
GLP-1 microdosing isn’t a weight-loss plan. Microdosing isn’t an FDA-approved dosing category. Lower-dose use should only be considered with help from a licensed provider who reviews the woman’s health history, goals, medications, risks, side-effect history, and current weight status.
At Josie, microdosing may come up in two main situations.
The first situation is tapering down after reaching a stable weight. After a provider-guided GLP-1 plan, some women may want help maintaining their progress instead of continuing to focus on active weight loss.
The second situation is starting from a comfortable weight. Some women aren’t trying to lose weight, but they notice midlife changes that make maintenance harder.
Both situations have the same center: maintenance, healthy habits, and provider guidance.
Josie microdosing isn’t used or discussed as a weight-loss plan.
Women seeking active weight loss should discuss standard GLP-1 treatment options with a licensed provider when clinically appropriate. Microdosing shouldn’t be positioned as a cheaper version of full-dose GLP-1 treatment, a hack to lose a few pounds, or a way to get GLP-1 results without standard treatment.
GLP-1 microdosing isn’t proven to extend lifespan, slow aging, prevent disease, or improve longevity markers. At Josie, longevity support means helping women maintain healthy habits and long-term weight stability. It doesn’t mean microdosing is proven to extend lifespan or prevent disease.
Lower-dose doesn’t mean side-effect-free. Some women may still experience nausea, constipation, bloating, fatigue, appetite changes, or digestive discomfort.
GLP-1 microdosing may be considered for some women who are focused on maintaining their weight, not losing weight.
This may include women who’ve reached a stable weight after a provider-guided GLP-1 plan. A licensed provider may review whether tapering down to a lower-dose maintenance approach fits their health history, current weight status, side-effect history, medications, and long-term goals.
GLP-1 microdosing may also be discussed for women who are already at a comfortable weight. These women may want support as midlife changes affect appetite, cravings, sleep, energy, recovery, muscle, body composition, weight stability, or routine consistency.
Microdosing may be a fit for women who want provider-guided support instead of self-adjusting. A licensed provider should review whether microdosing fits the woman’s health history, current weight status, medications, maintenance goals, and risk factors.
GLP-1 microdosing isn’t right for every woman because lower doses can still cause side effects, may not fit certain health histories, and aren’t designed at Josie for active weight loss.
Microdosing may not be appropriate for women seeking active weight loss. Those women should discuss standard GLP-1 treatment options with a licensed provider when clinically appropriate.
Microdosing may not be appropriate for women trying to self-dose without medical guidance. Dose decisions, tapering decisions, and medication changes should be reviewed by a licensed provider.
Microdosing may not be appropriate for women with health risks that require closer medical review, a history of significant side effects, medication interactions, complex health histories, pregnancy, plans to become pregnant, or breastfeeding. A licensed provider should review the risks, benefits, and alternatives before deciding whether any GLP-1 option may be appropriate.
Midlife can change how women think about tirzepatide, semaglutide, and GLP-1 microdosing because the goal may shift from losing weight to maintaining stability.
Some women in midlife aren’t trying to lose a large amount of weight. They’re trying to stay steady while appetite, cravings, sleep, energy, recovery, and body composition feel less predictable.
During perimenopause, menopause, and postmenopause, familiar habits may not feel as effective as they once did. Sleep may get lighter. Cravings may feel stronger. Recovery may take longer. Muscle can feel harder to maintain. Weight may creep up even when daily routines haven’t changed much.
That’s the setting where microdosing may come up at Josie. The goal isn’t to chase the lowest number on the scale. The goal is to support maintenance, consistency, and long-term habits during a changing season of life.
Longevity support at Josie means supporting habits and health patterns that may contribute to long-term wellness.
Longevity support may include maintaining a stable weight, staying consistent with strength training, building protein-focused nutrition habits, avoiding rebound weight gain after reaching a goal, and having proactive metabolic health conversations with a licensed provider.
Longevity support doesn’t mean GLP-1 microdosing extends lifespan. It doesn’t mean microdosing slows aging, prevents disease, works as an anti-aging treatment, or improves longevity markers without proof.
Microdosing may be one part of a broader maintenance conversation for some women. Nutrition, movement, sleep, strength, and provider-guided care remain the foundation.
Lean muscle matters during GLP-1 conversations because weight changes can affect body composition.
For midlife women, muscle supports strength, function, metabolism, balance, and long-term health. A maintenance plan shouldn’t focus only on the scale because body composition can change even when weight stays steady.
Protein-focused nutrition, resistance training, and realistic routines belong in the same conversation as medication. A licensed provider can help review whether a woman’s maintenance plan supports weight stability without ignoring strength, energy, or muscle.
Lower-dose GLP-1 use can still cause side effects.
Some women may experience nausea, constipation, bloating, fatigue, appetite changes, or digestive discomfort. A lower dose may mean lower medication exposure, but lower exposure doesn’t remove risk.
Side effects can depend on the medication, dose, health history, other medications, eating patterns, hydration, digestive sensitivity, and prior GLP-1 experience.
A licensed provider should explain possible risks, benefits, and alternatives before deciding whether microdosing may be appropriate.
Microdosing isn’t an FDA-approved dosing category because FDA-approved GLP-1 medications are approved with specific labeled dosing schedules.
Those labels include studied starting doses, escalation schedules, maintenance doses, warnings, and instructions. Microdosing falls outside those labeled schedules.
FDA-approved GLP-1 medications follow labeled dosing schedules. Microdosing isn’t an FDA-approved dosing category, so it isn’t offered as a labeled brand-name dosing option.
Most microdosing conversations involve compounded versions because compounded preparations may allow different strengths, concentrations, or formats. That flexibility doesn’t make compounded GLP-1 medications FDA-approved.
Compounded GLP-1 medications aren’t FDA-approved and haven’t been evaluated by the FDA for safety, effectiveness, or quality.
Compounded GLP-1 medications aren’t FDA-approved.
The FDA hasn’t evaluated compounded GLP-1 medications for safety, effectiveness, or quality. Compounded preparations may differ in formulation, strength, concentration, or delivery method.
Compounded GLP-1 medications aren’t generic versions of brand-name GLP-1 medications. They shouldn’t be treated as equivalent substitutes for brand-name medications unless a licensed provider determines a commercially available product isn’t suitable for the patient.
Josie connects eligible patients with licensed providers. Josie isn’t the compounding pharmacy.
A licensed provider should explain the risks, benefits, and alternatives before deciding whether a compounded option may be appropriate.
Josie approaches GLP-1 microdosing as a provider-guided maintenance conversation for midlife women.
A licensed provider reviews the patient’s health history, current weight status, symptoms, goals, medications, side-effect history, and risk factors before discussing any medication option.
Some women may need a standard GLP-1 plan for weight-loss support when clinically appropriate. Some women may be better suited for a maintenance discussion. Some women may need a different care path entirely.
The goal is to match the conversation to the person. GLP-1 microdosing isn’t for everyone, and it shouldn’t be used as a DIY dosing strategy.
Microdosing Plans at Josie:
Patients must qualify through a Josie licensed provider. If appropriate, microdosing is for weight maintenance, not weight loss.
No large clinical trial evidence proves that tirzepatide is better than semaglutide for microdosing.
Tirzepatide works through both GIP and GLP-1 pathways. Semaglutide works through the GLP-1 pathway. That difference may affect how each medication feels, but microdose-level outcomes aren’t well established.
No large clinical trial evidence proves that semaglutide is better than tirzepatide for microdosing.
Semaglutide and tirzepatide work differently, and individual response can vary. A licensed provider should review the patient’s health history, current weight status, medications, side-effect history, and maintenance goals before discussing either option.
No. At Josie, GLP-1 microdosing isn’t used or discussed as a weight-loss plan.
GLP-1 microdosing is positioned for weight maintenance and longevity support when a licensed provider decides it may be appropriate. Women seeking active weight loss should discuss standard GLP-1 treatment options with a licensed provider.
GLP-1 microdosing may be considered for some women who are focused on maintaining their weight, not losing weight.
This may include women who’ve reached a goal weight or women who are already at a comfortable weight but want support with healthy habits during midlife.
Some women may discuss microdosing with a licensed provider even if they’re already at a comfortable weight.
At Josie, that conversation is about maintaining weight, supporting healthy habits, and navigating midlife changes. The goal isn’t chasing weight loss.
Some women may discuss tapering down after reaching a stable weight.
A licensed provider should review whether a lower-dose maintenance approach fits their health history, current weight status, side-effect history, medications, and long-term goals.
No. Microdosing isn’t an FDA-approved dosing category.
FDA-approved GLP-1 medications have labeled dosing schedules based on studied doses. Microdosing isn’t part of those labeled dosing schedules.
Compounded GLP-1 medications aren’t FDA-approved and haven’t been evaluated by the FDA for safety, effectiveness, or quality.
Brand-name GLP-1 medications don’t offer microdosing as a labeled dosing option because FDA-approved GLP-1 medications follow specific labeled dosing schedules.
Microdosing falls outside those labeled schedules. A licensed provider should explain the risks, benefits, and alternatives before deciding whether any lower-dose or compounded option may be appropriate.
Microdosing conversations often involve compounded versions because compounded preparations may allow different strengths, concentrations, or formats.
That flexibility can make lower-dose approaches possible in a way that fixed brand-name dose schedules usually don’t. Compounded GLP-1 medications aren’t FDA-approved and haven’t been evaluated by the FDA for safety, effectiveness, or quality.
Yes. Lower doses can still cause side effects.
Some women may experience nausea, constipation, bloating, fatigue, appetite changes, or digestive discomfort. A licensed provider should review side-effect history and risk factors before deciding whether microdosing may be appropriate.
At Josie, longevity support means supporting healthy habits and long-term weight stability.
Longevity support may include maintaining a stable weight, staying consistent with strength training, building protein-focused nutrition habits, avoiding rebound weight gain, and having proactive health conversations with a licensed provider.
GLP-1 microdosing isn’t proven to extend lifespan, slow aging, prevent disease, or work as an anti-aging treatment.
A licensed provider reviews the patient’s health history, current weight status, symptoms, goals, medications, side-effect history, and risk factors before discussing any medication option.
For women considering microdosing, the conversation centers on weight maintenance, longevity support, and healthy habits. The intake form helps gather information, but it isn’t a diagnosis or an automatic approval.
FDA. Compounding and the FDA: Questions and Answers.
https://www.fda.gov/drugs/human-drug-compounding/compounding-and-fda-questions-and-answers
FDA. Understanding the Risks of Compounded Drugs.
https://www.fda.gov/drugs/human-drug-compounding/understanding-risks-compounded-drugs
FDA. FDA’s Concerns With Unapproved GLP-1 Drugs Used for Weight Loss.
https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/fdas-concerns-unapproved-glp-1-drugs-used-weight-loss
FDA. WEGOVY Prescribing Information.
https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/215256s024lbl.pdf
FDA. ZEPBOUND Prescribing Information.
https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/217806Orig1s020lbl.pdf
New England Journal of Medicine. Once-Weekly Semaglutide in Adults with Overweight or Obesity.
https://www.nejm.org/doi/full/10.1056/NEJMoa2032183
New England Journal of Medicine. Tirzepatide Once Weekly for the Treatment of Obesity.
https://www.nejm.org/doi/full/10.1056/NEJMoa2206038
ClinicalTrials.gov. SURMOUNT-5: Tirzepatide vs. Semaglutide for Weight Management.
https://clinicaltrials.gov/study/NCT05822830
Medical disclaimer: This content is for educational purposes only and isn’t a substitute for professional medical advice. Individual results vary. Microdosing isn’t an FDA-approved dosing category. Compounded GLP-1 medications aren’t FDA-approved and may differ from branded products in formulation, strength, concentration, or delivery method. Compounded GLP-1 medications aren’t equivalent to and shouldn’t be considered substitutes for brand-name medications unless a licensed provider determines a commercially available product isn’t suitable. Microdosing hasn’t been evaluated in large randomized clinical trials. Josie is a telehealth platform that connects eligible patients with licensed providers. Josie isn’t the compounding pharmacy. Not every care option is right for every woman. A licensed provider reviews your health history, symptoms, and goals before recommending any care path. Common side effects with GLP-1 medications can include nausea, bloating, fatigue, and constipation. Serious adverse events are rare but possible. Always talk with a licensed healthcare provider about the risks, benefits, and alternatives before starting, stopping, or changing any medication.